ECR 2012 / C-1397
Arterial Embolization in Postpartum Hemorrhage
Congress:
ECR 2012
Poster Number:
C-1397
Type:
Educational Exhibit
Keywords:
Interventional vascular, Fluoroscopy, Embolisation, Haemorrhage
Authors:
A. Urquia1, J. ALDEA MARTINEZ2, L. Adrián Lozano2, J. L. López Martínez2, M. A. Castaño Blazquez3; 1Burgos, Ca/ES, 2BURGOS/ES, 3005/ES
DOI:
10.1594/ecr2012/C-1397

Fig. 3:
Initial materials used: 6 French arterial introducer Super Arrow-Flex® and...

Fig. 4:
Left: normal anatomy in an aortogram with internal iliac arteries and its...

Fig. 5:
Drawing of the arterial anatomy of the female tract.

Fig. 7:
Left: Uterine artery with its characteristic U-shaped course. Right: Enlarged...

Fig. 12:
Left: Right internal iliac artery previous to embolization.
Right:...

Fig. 11:
Coil, permanent embolic material.

Fig. 10:
Steps in the preparation of the embolic material, in this case, Surgicel, cut...
 (Cook; Bjaeverkov, Denmark).")
Fig. 9:
Left: Active extravasation of contrast and pseudoaneurysm of vesical artery....

Fig. 8:
Left: Superselective arteriography of right uterine artery.
Right:...

Fig. 13:
Vascular closure device Angio-Seal™ VIP

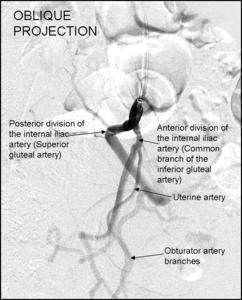
Fig. 6:
The origin of the uterine artery from the anterior division of the iliac artery...